For patients with recurrent pregnancy loss
Examination and causes of RPL
The four major causes of miscarriage are antiphospholipid syndrome (APS), a congenital uterine anomaly, chromosomal structural rearrangement in either partner, and fetal (embryonic) chromosomal aneuploidy (1, 4-6). Antiphospholipid antibodies are found in 10% of cases, chromosomal rearrangement abnormalities in 6%, and uterine malformations in 3.2% (Fig. 2-A). The prevalence of APS that meets the definition of the International Society for Antiphospholipid Antibodies is about 4% (6). Endocrine abnormalities include diabetes hypothyroidism, as well as polycystic ovary syndrome, but the latter is still controversial.
Figure 2:Distribution of causes of recurrent pregnancy loss
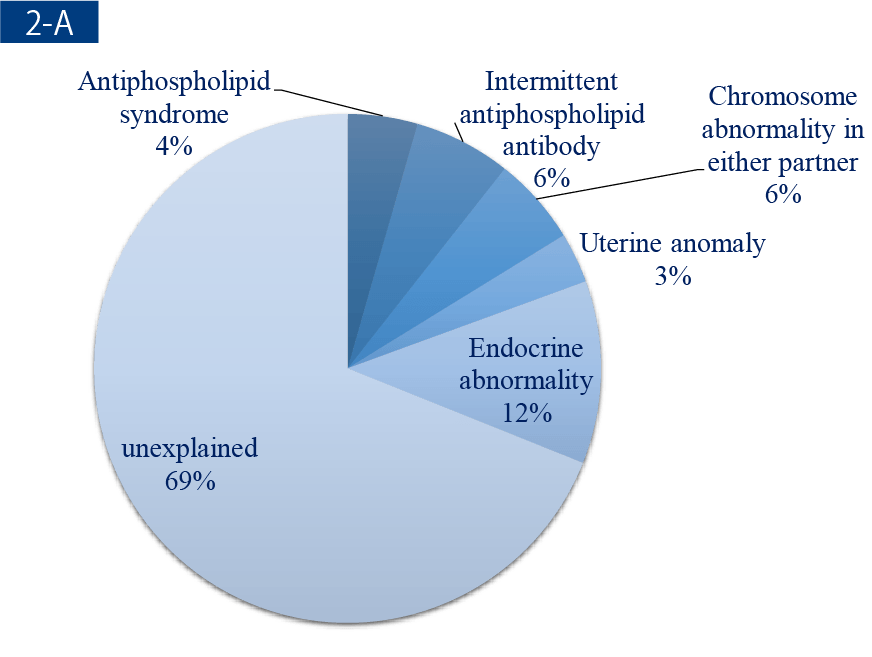
1676 couples
Sugiura-Ogasawara et al. Fertil Steril 2010
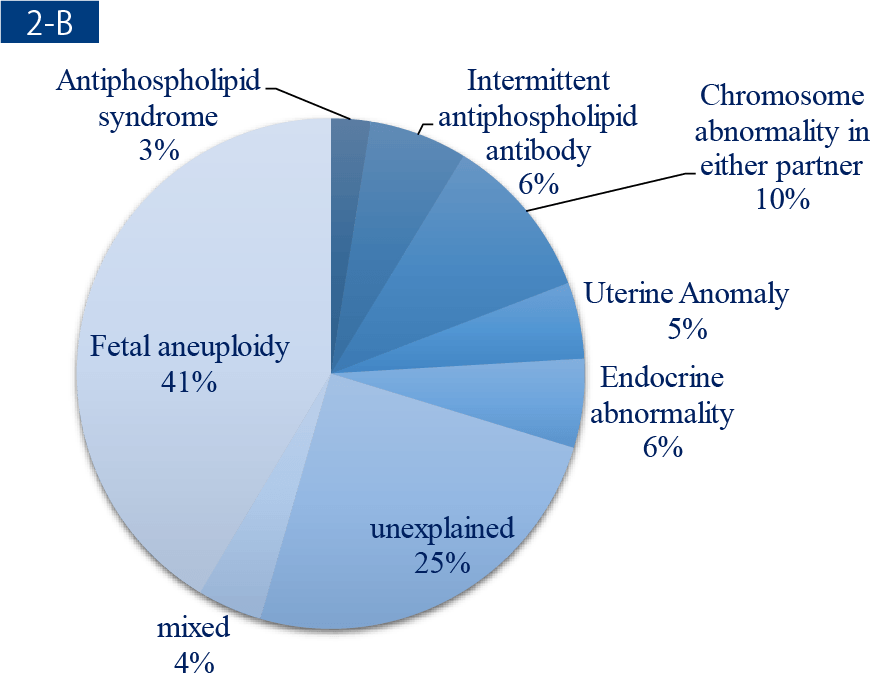
482 couples
Sugiura-Ogasawara et al. Hum Reprod 2012
The four major causes of RPL at this time are listed below (Table 3).
- Antiphospholipid syndrome
- Congenital uterine anomaly
- Chromosomal structural rearrangement in either husband or wife
- Fetal or embryonic chromosome aneuploidy
Because fetal chromosome testing is not covered by health insurance in Japan and can only be performed in a limited number of facilities, it is rarely performed on fetuses of past miscarriages in patients who come in for their first visit. Therefore, RPL of "unknown cause" comprised 69 % of the cases (Fig. 2-A). However, when properly examined, 41% of fetuses showed chromosome aneuploidy, a rate which increased with the age of the woman (Fig. 2-B, ref. 5). The frequency of cases with a truly unknown cause was about 25%. Recommended tests are listed in Table 3 and the details are explained item by item.
Table 3: Examination and management of patients with recurrent pregnancy loss
← Please see by side-scrolling →
| Causes | Examination | management |
|---|---|---|
| Antiphospholipid Syndrome |
|
|
| Congenital uterine anomaly | Ultrasound sonography |
|
| Chromosomal rearrangement abnormalities (Translocation) | Chromosome karyotype |
|
| Fetal or embryonic chromosome aneuploidy | Chromosome karyotype in products of aborted conception |
|
Index
- Definition of recurrent miscarriage and recurrent pregnancy loss and results of the Japan Environment and Children’s Study (JECS)
- Examination and causes of RPL
- Antiphospholipid syndrome
- ー
- Treatment of antiphospholipid syndrome
- Chromosomal translocation in either partner
- Preimplantation genetic testing for chromosomal structural rearrangement
- Congenital uterine anomaly
- Thrombotic predisposition
- Endocrine abnormality
- Fetal or embryonic aneuploidy
- Preimplantation genetic testing for aneuploidy
- Immunotherapy for unexplained recurrent miscarriage
- Drug administration for repeated miscarriages of unknown cause
- Unknown Causes
- Emotional support
- References
