For patients with recurrent pregnancy loss
Treatment of antiphospholipid syndrome
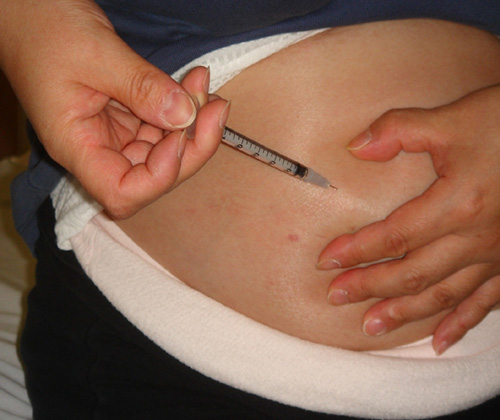
Low-dose aspirin and heparin therapy is the standard of care for the prevention of miscarriage, with a live birth rate of 70-80% (12, 13). With this therapy, we calculate the exact number of weeks of gestation based on the basal body temperature and bigin low-dose aspirin (Bufferin 81 mg® or Biaspyrin®) and heparin injections at 4 weeks of gestation, stopping aspirin at 36 weeks and 0 days of gestation, and continuing heparin until 3-6 hours before delivery. With training, self-injection of heparin is not difficult (photo). If the antiphospholipid antibodies are negative and antinuclear antibodies are positive, no medication is required..
Self-injection of heparin
When the diagnostic criteria were not met, e.g., a case in which the antiphospholipid antibodies were positive but became negative after 12 weeks, we looked at whether miscarriage prophylaxis was necessary (14). Comparing the aspirin alone group with 50.0% (8/16) positivity and the group given no medication, it was found that the aspirin group had a live birth rate of 84.6% (44/52) which was higher than the unmedicated group. However, similar reports have not yet emerged from Europe or the United States, and these findings may need to be re-examined.
A clinical trial was conducted using danaparoid (Orgaran®) to see how it compared with the unfractionated heparin used previously (15). Orgaran is known to have fewer side effects of bleeding, heparin-induced thrombocytopenia and osteoporosis, and was found to be as effective as unfractionated heparin. It is not covered by health insurance, but it is safe to use.
Index
- Definition of recurrent miscarriage and recurrent pregnancy loss and results of the Japan Environment and Children’s Study (JECS)
- Examination and causes of RPL
- Antiphospholipid syndrome
- ー
- Treatment of antiphospholipid syndrome
- Chromosomal translocation in either partner
- Preimplantation genetic testing for chromosomal structural rearrangement
- Congenital uterine anomaly
- Thrombotic predisposition
- Endocrine abnormality
- Fetal or embryonic aneuploidy
- Preimplantation genetic testing for aneuploidy
- Immunotherapy for unexplained recurrent miscarriage
- Drug administration for repeated miscarriages of unknown cause
- Unknown Causes
- Emotional support
- References
